


 Sign Out
Sign Out

Undesirable effects are for the most part dose-dependent. They are more frequent and more severe at the start of treatment and will usually diminish with continued treatment.
Movement disorders may occur, especially at the start of treatment. In the majority of cases these adverse reactions can be satisfactorily remedied by reducing the dose and/or using of antiparkinson agents. Routine prophylactic use of antiparkinson agents is not recommended. Antiparkinson agents do not relieve tardive dyskinesias, but can worsen the symptoms. Dose reduction or, if possible, discontinuation of therapy is recommended. A benzodiazepine or propranolol may be beneficial in patients with persistent akathisia.
Frequencies are taken from the literature and spontaneous reporting. Frequencies are defined as: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), or not known (cannot be estimated from the available data). (See table.)
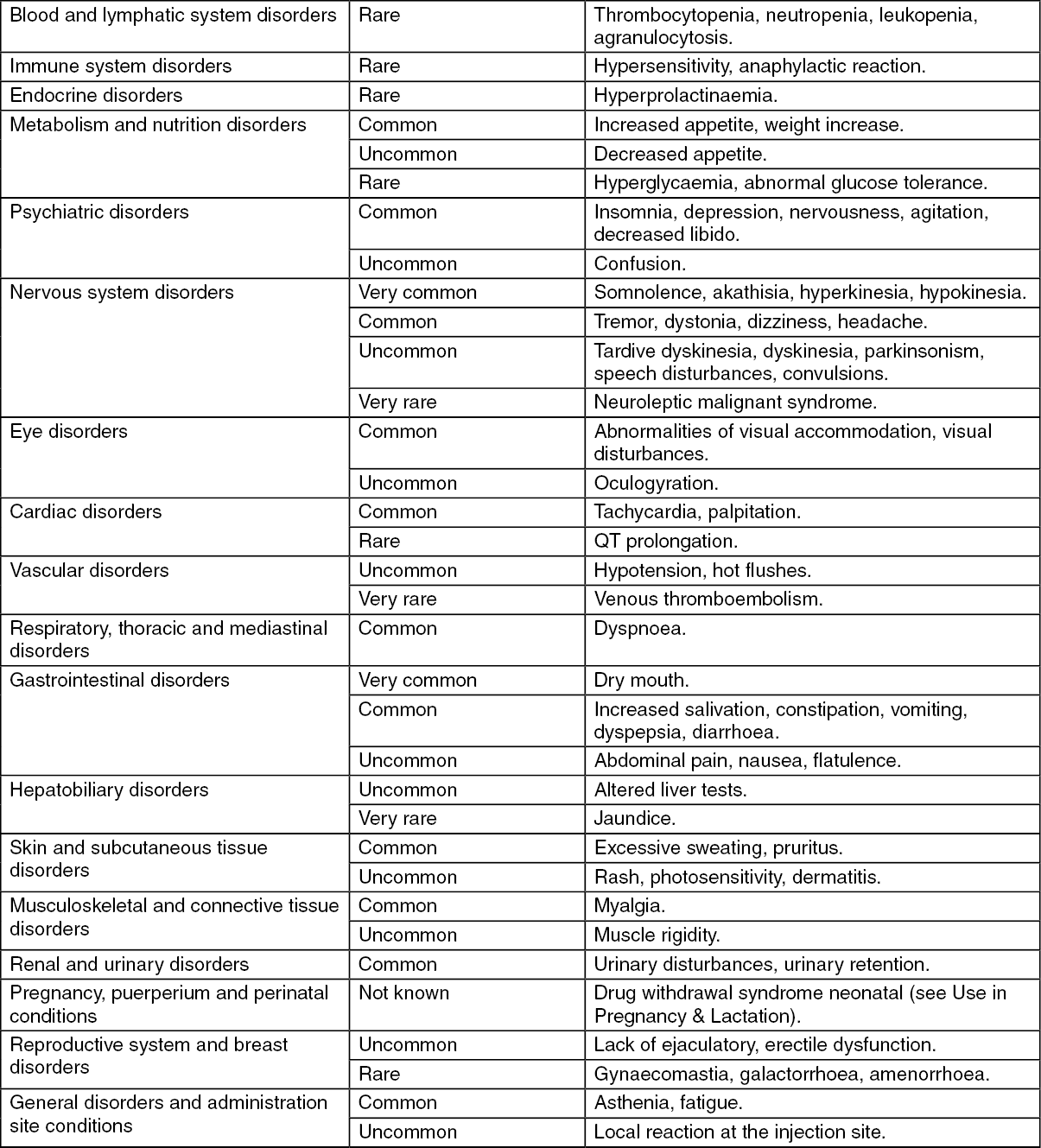 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAs with other antipsychotics, rare cases of QT prolongation, ventricular arrhythmias such as ventricular fibrillation and ventricular tachycardia, Torsade de Pointes and sudden unexplained death have been seen in connection with flupentixol (see Precautions).
Sudden discontinuation of flupentixol may give rise to withdrawal symptoms. The most common symptoms are nausea, vomiting, anorexia, diarrhoea, rhinorrhoea, sweating, myalgias, paraesthesias, insomnia, restlessness, anxiety and agitation. Patients may also experience vertigo, may feel warm/cold, respectively, and experience tremor. The symptoms usually set in 1-4 days after discontinuation and subside during 1-2 weeks.
View ADR Monitoring Form